
Five Sisters
A family's losses, a century of progress, and what evidence-based medicine owes to both.

As I ease towards retirement from clinical practice, I’ve been spending time revisiting cherished family heirlooms. Lately, I’ve been working on a series of letters between my paternal grandmother and her four sisters. Written in 1952, the letters recount growing up in rural western Iowa in the late 19th and early 20th centuries.
The five sisters reminisce about everyday life on the farm — filling tick mattresses, butchering hogs — the rhythms of a world that no longer exists. By today’s standards, theirs were difficult lives, but they seem to have been happy, until they lost both parents within a year of each other, leaving the girls orphaned at ages ranging from seven to twenty. Their subsequent lives were turbulent, but as one of the sisters puts it, “My childhood according to kids today was a mess but I lived thru it…”

From a medical perspective, their history is striking. In addition to the five sisters who survived, three other siblings died in infancy, and both parents died when quite young — a mortality rate of 50 percent in a single family.
One sibling is described as succumbing to “summer complaint” — a quaint but deceptive term for what we would now call acute gastroenteritis, typically caused by contaminated milk and poor sanitation, and peaking in summer months due to the absence of refrigeration. The cause of death of the other two infants is unspecified, but it is nearly certain they also fell prey to infectious disease, either gastrointestinal or respiratory.
Their mother, Sarah, died at 43 of a chronic illness of unspecified duration. She is described as having “spells,” typically in the evenings, that left her in a “stupor” the following day. She died either during one of those spells or shortly after, and her death seems to have been unexpected. Based on these limited descriptions, epilepsy seems the most likely diagnosis.
Their father, Henry, died a year later at 53. My grandmother, who later became a nurse, noted that he had “Bright’s Disease,” an older term for renal failure, and mentioned that she was surprised he didn’t “go into a coma,” by which she presumably meant a uremic coma. The likely culprits in that era were untreated chronic hypertension and post-streptococcal glomerulonephritis.
Three deaths from acute illnesses which were almost certainly preventable, and two from conditions that would be manageable, had this family lived a century later.
Thomas Hobbes, writing in Leviathan in 1651, described the life of man as “solitary, poore, nasty, brutish, and short.” Looking at this family’s history, it’s hard to argue with him — at least for their era.
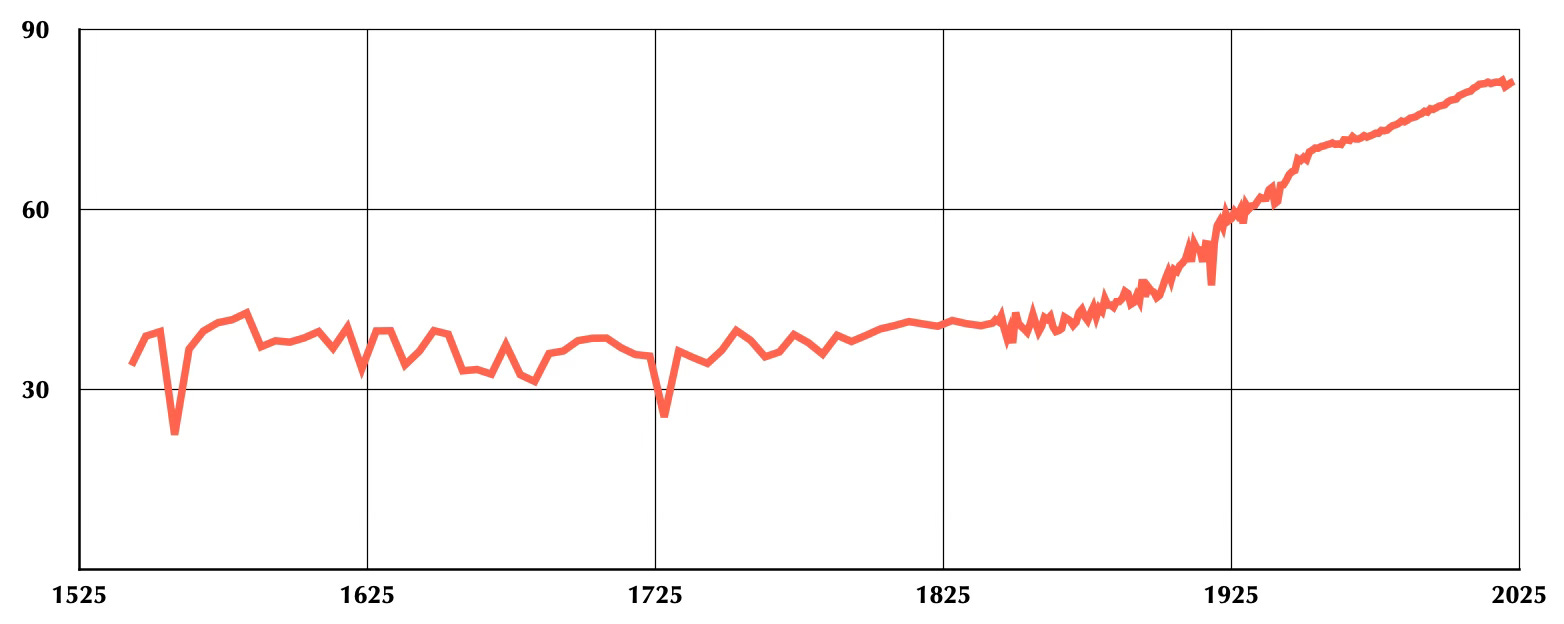
Life expectancy data from the United Kingdom, which has the oldest such records and tracks closely with U.S. data from the mid-19th century onward, shows centuries of average lifespans hovering between 35 and 40 years. Then, beginning around 1800, a sustained and dramatic rise.
What drove that rise is worth examining carefully, because the answer is not what most people assume.
It wasn’t, in the main, what we would call “modern medicine”, at least not at first. Much of the early improvement came from sanitation: cleaner water, better waste removal, and a growing public health sensibility that preceded formal acceptance of germ theory by decades. Pasteurization of milk became common in the United States in the early twentieth century, followed by widespread refrigeration. And while general anesthesia arrived in the 1840s, it would take another generation before surgeons reliably washed their hands before operating.
Edward Jenner established that inoculation with cowpox provided protection against smallpox in 1796. Other vaccines followed in the 20th century: diphtheria (1923), tetanus (1924), pertussis (1926), polio (1955), measles (1963). These were not small things.
Against that backdrop, “modern medicine” arrived quite late. Insulin, the first transformative non-vaccine medication, was used clinically for the first time in 1922. Penicillin became widely available only during World War II. Modern ventilators and cardiopulmonary bypass came in the 1950s. Dialysis for chronic renal disease, which might well have bought Henry many more years, didn’t become commonplace until the 1970s. CT scanning was routine by the 1980s; MRI followed a decade later.
What I inherited as a surgeon is, in its most meaningful sense, barely a century old. And much of what came before it — the sanitation revolution, the vaccines, pasteurized milk — is now so thoroughly taken for granted that we’ve largely forgotten it was ever an achievement.
Which brings me to where we are now.
If you look at that life expectancy curve, we appear to be at something of a plateau. I think that’s an accurate read. Through prevention and successful intervention, we have largely conquered the acute illnesses and injuries that claimed lives like those in this family. The low-hanging fruit has been harvested.
What remains is harder. Chronic diseases, such as cancer, heart disease, and dementia, may be manageable, and incremental advances likely. But dramatic breakthroughs are much more difficult, because the nature of progress has changed. Eradicating smallpox was huge, immediate, and visible. Its effects were obvious within a generation. The early gains of modern medicine came with large effect sizes, obvious benefits, and a simplicity of cause and effect that is genuinely rare now.
The trials we run today are different by necessity. We are working at the margins of diseases that are complex, chronic, and multifactorial. Effect sizes are smaller. Follow-up periods are longer. The signal is harder to separate from the noise — not because the science has gotten worse, but because the questions have gotten harder.
This is precisely why evidence-based medicine matters more today, not less. When the benefit is self-evident — when the child with diabetes gets insulin and lives — you don’t need a controlled trial. When a therapy offers a modest relative risk reduction in a surrogate endpoint over a five-year follow-up, rigorous methodology is the only reliable guide we have.
I’m reminded of what one of the sisters wrote, explaining why she wanted to set these memories down in the first place: “just so they are not laid aside and forgotten.” She was talking about farm life, about family, about a world that had passed. But I find myself thinking the same thing applies here. It is easy to take for granted what clean water, safe food, and effective vaccines have done for human health — precisely because those gains are now invisible, absorbed into the baseline of ordinary life.
The acute has been largely conquered. What lies ahead is the chronic, the incremental, the difficult to demonstrate. We should be clear-eyed about that — and hold the evidence to exactly the standard such difficulty demands.
In case anyone would like to peruse the letters from the five sisters:
This was a great read, thanks for sharing